
 AUD
AUD
 Loading... Please wait...
Loading... Please wait...

Recent Posts
Australia’s Greatest Public Policy Disaster Since 1915
Posted by on
Australia’s Greatest Public Policy Disaster Since 1915
When the dust settles in the years to come, much will be written about the COVID-19 pandemic and how the world came to terms with it.
This is particularly true of Australia where some of the most extraordinary and extreme public policy decisions have been made during the course of 2020 and 2021, some of which will have long-term detrimental generational impacts – especially as it relates to economic policy.
Millions of Australians have been shocked by the totalitarian decisions of the governments of New South Wales (NSW) and Victoria in particular which, without exaggeration, have deployed policies and tactics that are literally similar to the fascist and communist regimes which existed in 20th Century history.
The people of Australia were repeatedly told that:
- lockdowns;
- mask and vaccine mandates;
- house arrest under the guise of ‘self-isolation’ or ‘home quarantine’;
- state border closures;
- the suspension of civil and political rights;
- the inability to earn an income;
- deployment of the Australian Army; and
- police brutality (including the use of counter-terrorism resources)
were necessary and justified given the risks posed by COVID-19 – especially the “delta variant”.
To a large degree, a significant proportion of Australian citizens accepted and acquiesced to these policies given that they accepted the risk profile to public health as promoted by:
- mainstream scientists (especially epidemiologists and infectious disease experts);
- senior health bureaucrats (especially Chief Medical and Health Officers);
- political leaders;
- leading media and celebrity personalities; and
- relevant associated interest groups (such as business groups and trade union associations).
However, this assessment regarding the lethality of COVID-19 was not universal within the international scientific and medical community.
Indeed, as noted in the article, “Australia has been economically destroyed in 4 weeks”[1], which was published in April 2020:
- modelling controversies;
- questions regarding the accuracy of reverse transcription polymerase chain reaction (RT-PCR) testing; and
- observable data with respect to asymptomatic cases
suggested that the public health risk and potential lethality posed by COVID-19 was far lower than promoted by mainstream established political, scientific and medical authorities.
As the world has moved into the second-half of 2021, significant scientific and medical discoveries and insights with respect to COVID-19 have been uncovered which raise new questions as to the virus’ nature and how it should be managed.
These discoveries and insights raise new questions as to whether Australia’s management of COVID‑19 to date was justified and whether the current policy roadmap moving forward is appropriate.
As Australia (in particular NSW) moves forward to opening up its economy and society, it may well come to light that key scientific and medical assumptions which were at the centre of Australia’s policy approach were misguided and erroneous and thus the public policy response was dramatically both inappropriate and disproportionate.
If this is the case, the conclusion will be that the economic, social and psychological costs endured by the Australian people, in particular the people of NSW and Victoria, constitute an unparalleled unmitigated disaster on a scale not seen in Australian public administration since the catastrophic Gallipoli military campaign of 1915.
Importance of Virus Origination and Infection Model
To determine whether the management of the COVID-19 pandemic has been appropriate and proportionate, important linkages between the origin of COVID-19 and how it infects human populations need to be determined.
This is critical to understand, given that such linkages lead to important assumptions being made that form the basis of a wide sweep of public policy responses.
Australian scientists such as molecular immunologist Ted Steele[2] and his international group of research scientists, who have written extensively about the COVID-19 pandemic, believe that a comprehensive understanding of the infection model (i.e., how a virus infects and spreads throughout a human or animal population) is critical to determining the appropriate public health policy response.
In a recent public video, Steele stated[3] that any scientific hypothesis relating to COVID-19 must be able to both:
- comprehensively explain observed infection patterns; and
- accurately predict how COVID-19 is likely to behave in the future.
Moreover, Steele believes that a scientific understanding of the infection model of a virus cannot be divorced from the virus’ origins, given that the virus origin will provide important clues as to its molecular and genetic composition and how it behaves in general as well as in specific environments.
Defining the infection model of how a virus behaves becomes the basis for the formation of epidemiological modelling, which is then used to forecast the impact on public health if:
- no pandemic mitigation measures or controls are implemented; as well as
- certain mitigation measures or controls are implemented.
Such epidemiological modelling scenarios and forecasts then become the basis of designing and implementing the public policy response necessary to mitigate any public health risks posed by any virus.
The relationship between these linkages is outlined in Diagram 1.
Diagram 1: Relationship between the COVID-19 Infection Model and Public Policy Response

What is important to draw out from Diagram 1 in the context of both COVID-19 and Australia is that, if Australian epidemiologists and infectious disease experts have misunderstood the infection model of the COVID‑19 virus, then the subsequent epidemiological modelling and public policy response will be flawed – potentially by a materially significant degree.
Under such conditions, affected interest groups such as businesses and citizens may experience significant and irreversible net financial and non-financial costs.
Observed Virus Infection Patterns
Importantly, the nature of how viruses (including coronaviruses and Influenza) and bacteria infect human and animal populations has been subject of much scientific, medical and even theological discussion throughout history across multiple civilisations, empires, dynasties and geographies given the myriad epidemics and pandemics of our past.
Over the course of the past 700 years in Europe particularly, two prominent theories have been put forward regarding how viruses and bacteria spread. These theories include:
- a person-to-person (P-P) or animal-to-person (A-P) infection model; and
- a miasma (or atmospheric) infection model.
Interestingly, and as noted by Hoyle and Wickramasinghe (1979) in their seminal book, “Diseases from Space”[4], medieval European doctors subscribed to the miasma theory:
“Yet medieval doctors had no such thoughts. It was their overwhelming view that the pestilence had its origin in the air – ‘poisoned’ air was the widely favoured explanation.”
Alternatively, as noted by Hoyle and Wickramasinghe, it was doctors from India who first subscribed to the P‑P/A-P infection model:
“The first definite reference to plague occurs in the Bhagavata Purana, an Indian medical treatise written in the fifth century. There is a clear warning for people to leave their houses ‘when rats fall from the roofs above, jump about and die.”[5]
While the P-P/A-P infection model has, as noted by Hoyle and Wickramasinghe, become an ‘axiom’[6] in epidemiology, advocates of the miasma infection theory were still prominent during the 19th Century such as British epidemiologist Charles Creighton.
Again, as noted by Hoyle and Wickramasinghe:
“As recently as 1894 the distinguished British epidemiologist Charles Creighton, maintained that influenza was not an infectious disease. Citing medical opinion during the epidemic of 1833, 1837 and 1847, which held that the disease affected the entire country during the same one or two weeks, Creighton suggested that influenza was due to a ‘miasma’ spreading over the land rather than a disease that must spread by passing from person to person.”
It is within this context that COVID-19 must be critically considered and assessed. This is especially so given that the primary COVID-19 origination theories include:
- Theory 1 - COVID-19 originated from animals such as bats or pangolins;
- Theory 2 - COVID-19 originated from the Wuhan Institute of Virology – either deliberately or accidently leaked - as either ‘gain of function’ or biological weapons of mass destruction research; or
- Theory 3 - COVID-19 originated from an asteroid which struck the atmosphere above central China on 11 October 2019 (this theory is known as panspermia).
Specifically, a series of reported phenomena that have been observed during the current pandemic remains unexplained by conventional scientific explanations. These phenomena include:
- dramatic and sudden exponential growth of COVID-19 cases in particular cities and countries along the 40-degree latitude line in the Northern Hemisphere including Wuhan (China), Qom (Iran)[7] (approx. 19 February 2020[8]), Lombardy and Veneto (Italy) (approx. 25 February 2020[9]) and New York City (USA)[10] (approx. from 1 March to 22 March 2020)[11];
- on deck ship crew who tested negative for COVID-19 before they left port and who had no interactions with other ships at sea suddenly became struck with COVID-19 within a 24 - 48 hour period[12] - specific examples include the Diamond Princess, Grand Princess, USS Theodore Roosevelt and the Al Kuwait[13];
- humans on isolated islands becoming struck with COVID-19 as was the case with Chilean O’Higgins Army Outpost in Antarctica where most of the personnel were struck down suddenly and simultaneously with COVID-19 in late Dec 2020[14];
- the observance of COVID-19 mystery cases (i.e., COVID-19 infection cases that cannot be attributed to an originating patient) as observed in the case of Victoria, Australia[15];
- COVID-19 case counts that largely reflect symmetrical bell curves irrespective of public health interventions such as social distancing, lockdowns, mask mandates, deployment of vaccines, etc[16]; and
- the observance of ‘null zones’ – geographical areas and cities such as Hobart, Adelaide or Perth in the case of Australia which have not experienced rapid surges of COVID-19 daily infections during the course of the current pandemic.
Importantly, such patterns as described above have been observed in previous epidemics and pandemics throughout recent centuries. As noted by Hoyle and Wickramasinghe[17], in the case of the “Black Death” in Europe, isolated and remote villages in England were struck by the bubonic plague, while continental European cities such as Nuremberg, Milan and Liege were relatively untouched.
Hoyle and Wickramasinghe also noted that, in the context of the 1918-19 Spanish Flu pandemic, Alaska’s isolated villages were struck by a large outbreak of Spanish Flu in November/December 1918 despite their primitive modes of transportation (sleds and dogs) and that birds had already flown south given cold temperatures emanating from the onset of the winter season. Specifically, Hoyle and Wickramasinghe noted:
“The rapid spread of influenza across the frozen wasteland of Alaska in November/December 1918 remains a mystery on the basis of person-to-person transmission. With a population of 50,000 people very thinly spread over an area the size of Europe and with ground transportation essentially impossible, the only route of viral transfer must have been through the air.”
Moreover, Hoyle and Wickramasinghe also noted that, during the 1918-19 Spanish Flu pandemic, some isolated ships at sea (prior to the establishment of the global commercial aviation industry) were also suddenly struck with outbreaks of Spanish Flu:
“In other words, the passengers and crews of many ships at sea, totally isolated from infected persons, quite suddenly were afflicted whereas others were spared.”
Doherty Institute Modelling
Importantly, in the Australian context, the public policy response pursued by the Australian Government as well as the State and Territory Governments has been driven by modelling produced by the Melbourne-based Doherty Institute.
This modelling was dubbed by Australian Prime Minister Scott Morrison as the “National Plan”[18] and has been endorsed by the so-called “National Cabinet”[19] (a committee consisting of the Prime Minister and all State Premiers and Chief Ministers).
The National Plan involves a 4-stage road map which seeks to restore Australia to a pre-pandemic economic environment that is open to the world.
The essence of the plan is for Australian policy makers to implement draconian lockdowns where outbreaks of COVID-19 occur in order to “suppress” community COVID-19 transmission.
Such lockdowns are based on the premise that the infection model of the COVID-19 delta variant is based on rapid P-P community transmission.
Under the Doherty Institute modelling, the implementation of such lockdowns would continue until certain vaccination coverage thresholds are met sufficient for the Australian economy and society to unlock and open-up as safely as possible, assuming low levels of COVID-19 infection cases.
The basis of the Doherty Institute modelling is that once an Australian state or territory opens up, COVID-19 cases would rapidly increase as people mobility increased, however high vaccination coverage is assumed to ensure that mass severe illness or death resulting from COVID-19 would be contained or minimised.
Shockingly, in producing its modelling for National Cabinet, the Doherty Institute made no specific assumptions about the origins of COVID-19 and did not attempt to reconcile its model to the observed phenomena as mentioned above.
Expectations in NSW
Importantly, it is the P-P infection model assumed by the Doherty Institute which has shaped the epidemiological modelling produced by the NSW Health Department and the cautious 3-phase opening roadmap of the NSW Government.
As outlined by the former NSW Premier Gladys Berejiklian at her 20 September 2021 press conference[20], the opening up of NSW at vaccination thresholds of 70%, 80% and 90% are expected to result in new COVID-19 cases going “through the roof” and subsequently leading to the NSW Health system being "technically overwhelmed" with increased COVID-19 related hospitalisations and ICU admissions.
This expectation was also reiterated by NSW’s new Premier Dominic Perrottet in his press conference held on 9 October 2021[21].
Importantly, such is the concern of what opening up NSW may mean to public health that Nowra based Surgeon, Professor Martin Jones, went public on 7 October 2021 to state that “thousands of people” could potentially die in NSW directly from ending the COVID-19 related lockdown restrictions[22].
Similar concerns have also been expressed by the NSW President of the Australian Medical Association[23] as well as prominent Australian epidemiological academic professors, such as University of Melbourne Professor Anthony Blakely and Burnet Institute Professor Mike Toole, as reported by journalist Finbar O’Mallon in the Australian Financial Review on 11 October 2021[24].
Contrary Data
Critically, the European country of Norway has displayed an infection pattern which is at odds with the modelling from the Doherty Institute and NSW Health.
On 25 September 2021 at 4pm local time[25], the Norwegian Government abandoned all forms of COVID-19 related restrictions and opened up their country after an 80% double dose vaccination coverage was reached.
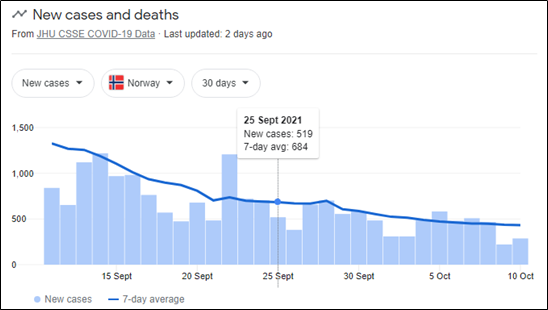
While such abandonment led naturally to an increase in people mobility, total COVID-19 cases and daily new cases in Norway actually fell by over 40% and 50% respectively[26], contrary to the underlying assumption underpinning the Doherty Institute and NSW Health epidemiological modelling.
This can be confirmed by observing data from John Hopkins University as displayed in Diagram 2.
Diagram 2: New COVID-19 Cases in Norway as of 10 October 2021
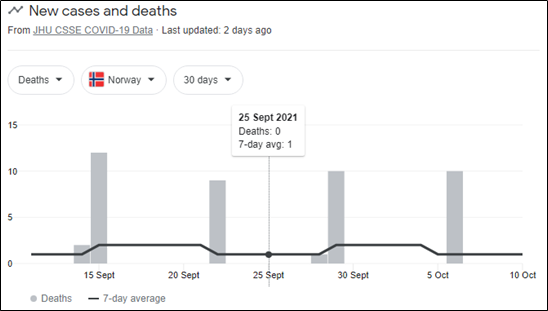
Moreover, the removal of COVID-19 restrictions saw that there was no observed increase in deaths in Norway as measured by the 7-day rolling average. From 25 September 2021 through to 10 October 2021, deaths resulting from COVID-19 on a 7-day rolling average was only 1 death per day.
This can be confirmed by observing data from John Hopkins University as displayed in Diagram 3.
Diagram 3: New COVID-19 Cases in Norway as of 10 October 2021
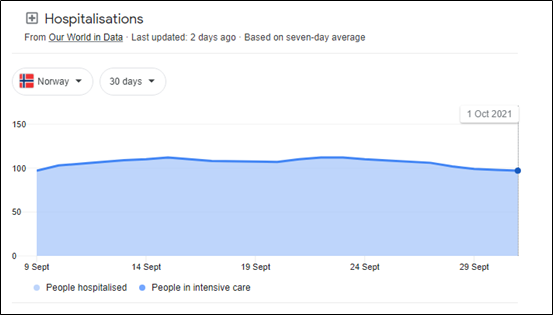
The stability in the death rate was also confirmed in Norway’s COVID-19 related hospitalisation rate which was also stable in the period after Norway removed its COVID-19 restrictions.
This can be confirmed by observing data from the “Our World In Data” series as displayed in Diagram 4.
Diagram 4: COVID-19 Hospitalisations as of 1 October 2021
With respect to COVID-19 cases in Norway, while a decline in recorded cases was observed for the two weeks since the end of restrictions on 25 September 2021, it is important to note that the number of tests also declined.
This can be confirmed by observing data from the “Our World in Data” series as displayed in Diagram 5.
Diagram 5: COVID-19 Daily Tests in Norway as of 5 October 2021
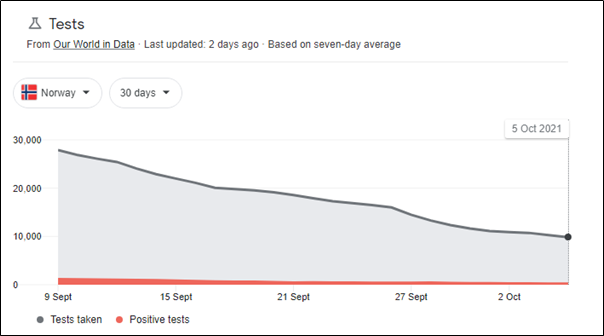
Importantly, while the number of total and new COVID-19 cases declined in Norway, the rate of COVID-19 tests shown to generate a positive test result grew slightly from 4.1% to 4.8% over the period from 25 September 2021 to 5 October 2021 as displayed in Table 1.
Table 1: The percentage of positive COVID-19 Daily Tests in Norway
| 25 September 2021 | 5 October 2021 | |
| Tests | 16,487 | 9821 |
| Cases | 676 | 471 |
| % of tests found to have positive COVID-19 cases | 4.1% | 4.8% |
While the slight increase in the number of COVID-19 tests yielding a positive result, this increase is hardly material when considering hospitalisation and death rates resulting from COVID-19 in Norway.
This slight increase again is at odds with the central premise of the epidemiological modelling from the Doherty Institute and NSW Health which predicts that cases, hospitalisation and ICU admissions are expected to dramatically increase as a result of increased mobility resulting from a P-P infection model.
Possible Explanation for Norway?
Given that Norway is at odds with the conventional epidemiological COVID-19 explanation, it is critical to consider if any possible explanations can be found to explain the Norwegian case study.
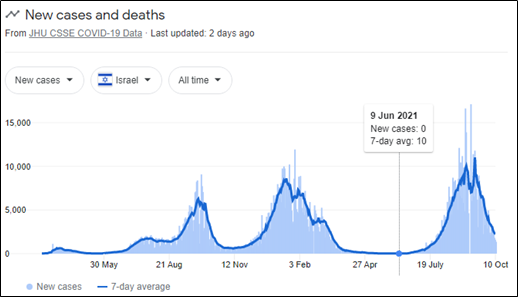
Importantly, Norway’s high rate of vaccination cannot be one of these explanations given counterfactual evidence from both Israel and Singapore.
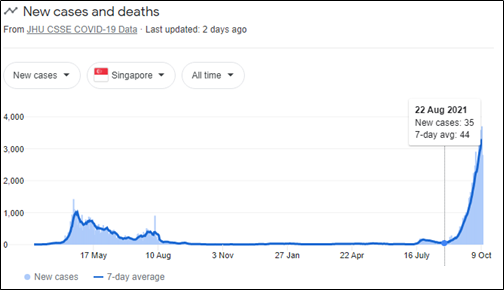
In both countries, the number of new daily COVID-19 cases reached their highest peak for the pandemic after a vaccination coverage over 80% was reached for citizens over 12 years old. In the case of Israel, the 80% coverage was reached in late August 2021[27] whereas in Singapore the 80% coverage was reached in early September 2021[28].
However, as illustrated in Diagram 6 with data from John Hopkins University, Israel had a 7‑day rolling average of new daily cases of only 10 on 9 June 2021 and then peaked at an all-time high for the pandemic at 16,629 new daily cases on 1 September 2021 or 9,308 cases on a 7-day rolling average basis.
Importantly, new daily cases in Israel have fallen (and continue to fall) as sharply as they rose in an almost symmetrical normal distribution (as noted above as one of the observed phenomena during the COVID-19 pandemic).
Diagram 6: New COVID-19 Cases in Israel as of 10 October 2021
Alternatively, in Singapore where the 7-day rolling average of new cases was 44 on 22 August 2021, new daily COVID-19 cases have now exploded to 2,809 cases as of 10 October 2021 and 3,303 cases on a 7-day rolling average.
Diagram 7: New COVID-19 Cases in Singapore as of 10 October 2021
Implications for NSW
In the context of NSW, the scientific assumption that COVID-19 spreads through a P-P infection model is about to be put to the test given that NSW officially, partially, emerged from lockdown on Monday, 11 October 2021. The staged unlocking of the NSW economy and society is because those 16 years and older reached the 70% double dose vaccination threshold in the previous week.
On the basis of the available data from NSW ending 8pm on Sunday, 10 October 2021, the evidence suggests to date that a P-P infection model is not at play in NSW.
During the current lockdown, which commenced in late June 2021, the typical symmetrical normal distribution which has been noted above and detailed by scientists who subscribe to miasma theory of infection such as Hoyle, Wickramasinghe and Steele has been observed for daily COVID-19 cases, hospitalisation and ICU admissions.
As noted in Diagrams 8 - 11, after a sharp rise in:
- total new COVID-19 daily cases;
- the percentage of COVID-19 tests that are positive;
- COVID-19 related hospitalisations; and
- COVID-19 related ICU admissions
all of these are now in sharp decline even though the NSW Government implemented a moderate lifting of lockdown restrictions (e.g., the lifting of curfews in Local Government Areas of concern and allowing vaccinated citizens to recreationally congregate in outdoor settings) in late September ahead of the official unlocking of NSW on 11 October 2021.
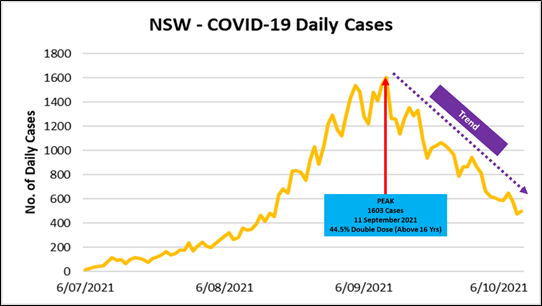
Importantly, as noted by the case studies of Israel and Singapore the rapid rollout of the COVID-19 vaccination program (which in NSW primarily consists of the Astrazenca and Pfizer vaccines) cannot be attributed to the observed phenomenon in NSW.
Specifically, as shown in Diagram 8, new daily COVID-19 cases in NSW peaked at 1603 cases on 11 September 2021 at a 44.5% double dose vaccination rate prior to falling to under 500 new daily infections for the 24 hours to 8pm ending on 10 October 2021.
Diagram 8: New COVID-19 Cases in New South Wales as of 8pm, 10 October 2021
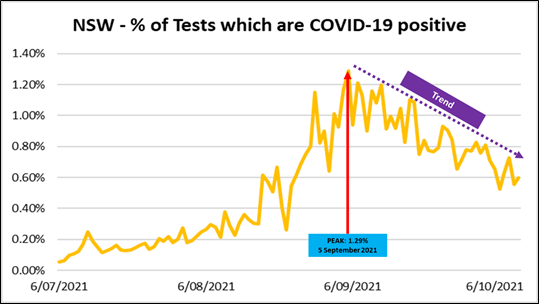
This relationship is also true when accounting for the level of COVID-19 testing. As shown in Diagram 9, the percentage of COVID-19 tests that yielded a positive result peaked on 5 September 2021 at 1.29% before falling by more than 50% to 0.6% in the 24 hours to 8pm on 10 October 2021.
Diagram 9: Rate of positive COVID-19 tests in New South Wales as of 8pm, 10 October 2021
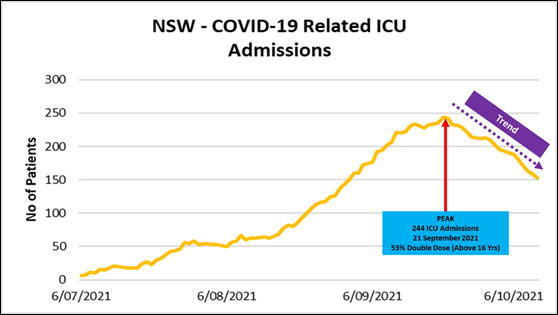
Importantly, with respect to severe COVID-19 illness, both hospitalisation (as shown in Diagram 10) and ICU admissions (as shown in Diagram 11) peaked on 21 September 2021 at 1266 hospital admissions and 244 ICU admissions respectively – 10 days after the case peak and 16 days after the peak in positive PCR test ratio – which coincided with a double dose vaccination coverage rate of 53% for citizens above the age of 16.
Diagram 10: COVID-19 Hospitalisations in New South Wales
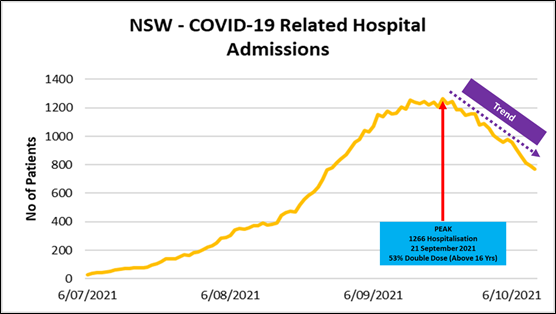
Diagram 11: COVID-19 related ICU Admissions in New South Wales
Given the graphical representation above, the coming 4 – 8 weeks will be critical to determining whether:
- the P-P or the miasma infection model is better suited to describing the COVID-19 epidemiological observed patterns in NSW;
- modelling produced by the Doherty Institute and NSW Health was based on the best available epidemiological theory and scientific evidence; and
- the extreme and totalitarian public policy response implemented by Australia’s governments based on the “National Plan” and the enormous economic, social and psychological costs experienced by the Australian people was appropriate, proportionate and justified to mitigate the public health risks posed by the COVID-19 pandemic.
Conclusion
While Australia and the world continue to battle COVID-19 and the consequences resulting from the global policy response, key scientific questions remain unanswered.
The most pressing key scientific questions, which are the most controversial, are these:
- 1.What is the infection model which best describes the epidemiological properties of COVID‑19?
- 2.Which model of the virus’ origin best contributes to determining the most appropriate infection model?
Conventional scientists around the world have blindly assumed that COVID-19 transmits via a P-P infection model. This assumption has subsequently influenced epidemiological public health modelling and the resulting public policy response which attempts to mitigate the public health risk posed by COVID-19.
In the Australian context, COVID-19 scientific controversies should be of major concern to both policy makers and citizens alike given the potential that public health measures implemented to date may be derived from a false epidemiological understanding of COVID‑19.
On the current evidence, both internationally and from NSW specifically, the miasma infection model theory appears to provide the complete understanding of observed phenomena meaning that lockdowns, social distancing and potentially ‘jab in the arm’ vaccines are, and have been, completely inappropriate public health measure responses.
Given:
- the enormous personal toll endured by the Australian people;
- the immense damage to Australia’s international reputation due to its governments embracing totalitarian public health measures; and
- the unsustainable explosion in Australia’s public sector debt and national money supply (via the Reserve Bank of Australia)
it would not be a radical statement to claim that the response to COVID-19 if based on a misguided and erroneous epidemiological understanding is the greatest disaster in Australian public administration since the 1915 catastrophic military campaign of Gallipoli.
John Adams is the Chief Economist of As Good As Gold Australia
[1]https://www.adamseconomics.com/post/australia-has-been-economically-destroyed-within-4-weeks
[2]https://en.wikipedia.org/wiki/Edward_J._Steele
[3]https://www.youtube.com/watch?v=Ijc4mjiIquk&feature=youtu.be
[4] Hoyle F., and Wickramasinghe C., (1979), “Diseases from Space”, J.M. Dent and Sons Ltd, United Kingdom
[5] See footnote 4
[6] An axiom can be defined as a statement or proposition which is regarded as being established, accepted, or self-evidently true.
[7]https://www.bbc.com/news/world-middle-east-51614920
[8] https://www.bbc.com/news/world-middle-east-51563039
[9] https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667(20)30099-2/fulltext
[10] Wickramasinghe, Steele, Gorczynski et al (2020) Virology Current Research Predicting the Future Trajectory of COVID-19. Virology Current Research Volume 4:1,2020 DOI DOI: 10.37421/Virol Curr Res.2020.4.111
[11] https://www.news10.com/news/covid-one-year-later-march-13-23-2020-timeline/
[12] Howard, GA, Wickramasinghe, NC, Rebhan, H et al (2020) Mid-Ocean Outbreaks of COVID-19 with Tell-Tale Signs of Aerial Incidence Virology Current Research Volume 4:1,2020 DOI: 10.37421/Virol Curr Res.2020.4.114
[13] Steele, E.J., Gorczynski ,R.M,. Rebhan, H., Carnegie, P., Temple, R., Tokoro, G., et al (2020) Implications of haplotype switching for the origin and global spread of COVID-19 Virol Curr Res Volume 4:2, 2020 DOI: 10.37421/Virol Curr Res.2020.4.115
[14] Steele EJ, Gorczynski RM, Lindley RA,Tokoro G, Wallis DH,Temple, Wickramasinghe NC Cometary Origin of COVID-19 (2021) DOI: 10.31038/IDT.2021212, https://researchopenworld.com/cometary-origin-of-covid-19/
[15] Lindley RA, Steele EJ. 2021 Analysis of SARS-CoV-2 haplotypes and genomic sequences during 2020 in Victoria, Australia, in the context of putative deficits in innate immune deaminase anti-viral responses. Scand J Immunol. 2021;00:e13100
[16] See footnote 13.
[17] See footnote 4.
[18]https://www.pm.gov.au/sites/default/files/media/national-plan-060821_0.pdf
[19] A recent decision by his Honour Justice Richard White of the Federal Court of Australia ruled that the “National Cabinet” is not a real cabinet in the traditional parliamentary Westminster system. Further information can be obtained from the following link: https://www.afr.com/politics/federal/secrecy-laws-don-t-apply-to-national-cabinet-judge-20210805-p58g9n
[20]https://www.abc.net.au/news/2021-09-20/nsw-records-935-covid-19-infections-and-four-deaths/100475524
[21]https://www.youtube.com/watch?v=eyPLKYs8nJ8
[22]https://www.camdencourier.com.au/story/7460400/surgeon-paints-grim-picture-of-nsws-covid-reopening/
[23]https://www.dailymail.co.uk/news/article-10070313/AMA-NSW-President-worries-opening-quickly-overwhelm-hospitals-warms-premier.html
[24]https://www.afr.com/policy/health-and-education/cases-will-rise-as-nsw-opens-the-question-is-by-how-much-20211011-p58yyx
[25]https://www.abc.net.au/news/2021-09-26/norway-lifts-covid-19-restrictions/100492390
[26] https://www.news.com.au/world/coronavirus/global/covid-cases-plunge-after-norway-abruptly-gets-rid-of-all-restrictions/news-story/d8c810f94ad5d6a5448dd03ac7d09ae0
[27]https://theconversation.com/covid-cases-are-rising-in-highly-vaccinated-israel-but-it-doesnt-mean-australia-should-give-up-and-live-with-the-virus-166404
[28]https://www.abc.net.au/news/2021-09-13/singapore-has-80-per-cent-vaccination-but-life-is-not-normal/100450154